Researchers explored metformin with or without rapamycin as maintenance therapy in patients with metastatic pancreatic adenocarcinoma.
Maintenance chemotherapy has previously been recommended for patients with metastatic pancreatic ductal adenocarcinoma (mPDA)—as PDA is an aggressive cancer at all stages, and treatment options are limited for later-stage mPDA. However, maintenance chemotherapy regimens often lead to toxicity and are not viable long-term options. Therefore, researchers are exploring alternative maintenance therapies for mPDA patients. In preclinical studies, the therapeutic combination of metformin and rapamycin demonstrated a potential synergy of anti-tumor activity in PDA.
“A synergistic effect of the combination of metformin with rapamycin was suggested by preclinical studies demonstrating enhanced inhibition of mTOR in a pancreatic cancer cell line and better growth inhibition of pancreatic cancer cells in a xenograft tumor model with the combination than either agent alone [21].”
Metformin is an antihyperglycemic drug that is frequently prescribed for patients with diabetes to help control blood sugar levels. Rapamycin is an immunosuppressive drug that has historically been prescribed to prevent organ rejection in kidney transplant patients. (Today, rapamycin is also being considered for its potential use in anti-aging and longevity interventions.) In animals, metformin and rapamycin both inhibit the major biological regulator of growth, named the mammalian target of rapamycin (mTOR). mTOR is thought to be a main driver of many (if not all) aging-related diseases, including cancers such as PDA.
“Mechanistic/mammalian target of rapamycin (mTOR) is a serine/threonine protein kinase which acts as a signaling node downstream of several oncogenic pathways including KRAS/MEK/ERK and PI3K/Akt, both of which are thought to be relevant drivers in a majority of PDAs [6–9].”
The Study
Given its promising potential, researchers—from Johns Hopkins University School of Medicine, Virginia Piper Cancer Center at HonorHealth, Translational Genomics Research Institute (TGen), and Shanghai Jiao Tong University School of Medicine—conducted a study exploring metformin, plus or minus rapamycin, in patients with metastatic PDA. Their priority research paper was published by Oncotarget in 2020, and entitled, “An exploratory study of metformin with or without rapamycin as maintenance therapy after induction chemotherapy in patients with metastatic pancreatic adenocarcinoma”.
A total of 22 unselected patients with mPDA were included in this randomized open-label phase 1b study between June 2014 and December 2017. Patients were at least 18 years of age and had previously been treated with chemotherapy for mPDA. At the beginning of the study, patients had either stable mPDA or responding mPDA for at least six months after induction chemotherapy. Half of the patients were randomly assigned to study Arm A, and the other 11 patients were assigned to study Arm B. Of note, the average age of the participants in Arm B was older (52–72; 66) than the participants in Arm A (34-73; 58). Otherwise, baseline characteristics between the study groups were relatively well-balanced.
Participants in study Arm A were assigned to take 850 milligrams of metformin orally, two times per day, for at least 12 months. Participants in study Arm B were assigned to take metformin and four milligrams of rapamycin once per day, for at least 12 months. The researchers conducted PET/CT scans, immunologic and metabolic analyses, statistical analysis, and continuously recorded and monitored for safety, patient tolerance, toxicity, and treatment-related adverse events.
“Treatment was continued until disease progression, intolerance of study treatments, or study closure, which occurred only after all remaining patients received a minimum of 12 months of treatment.”
Results and Conclusion
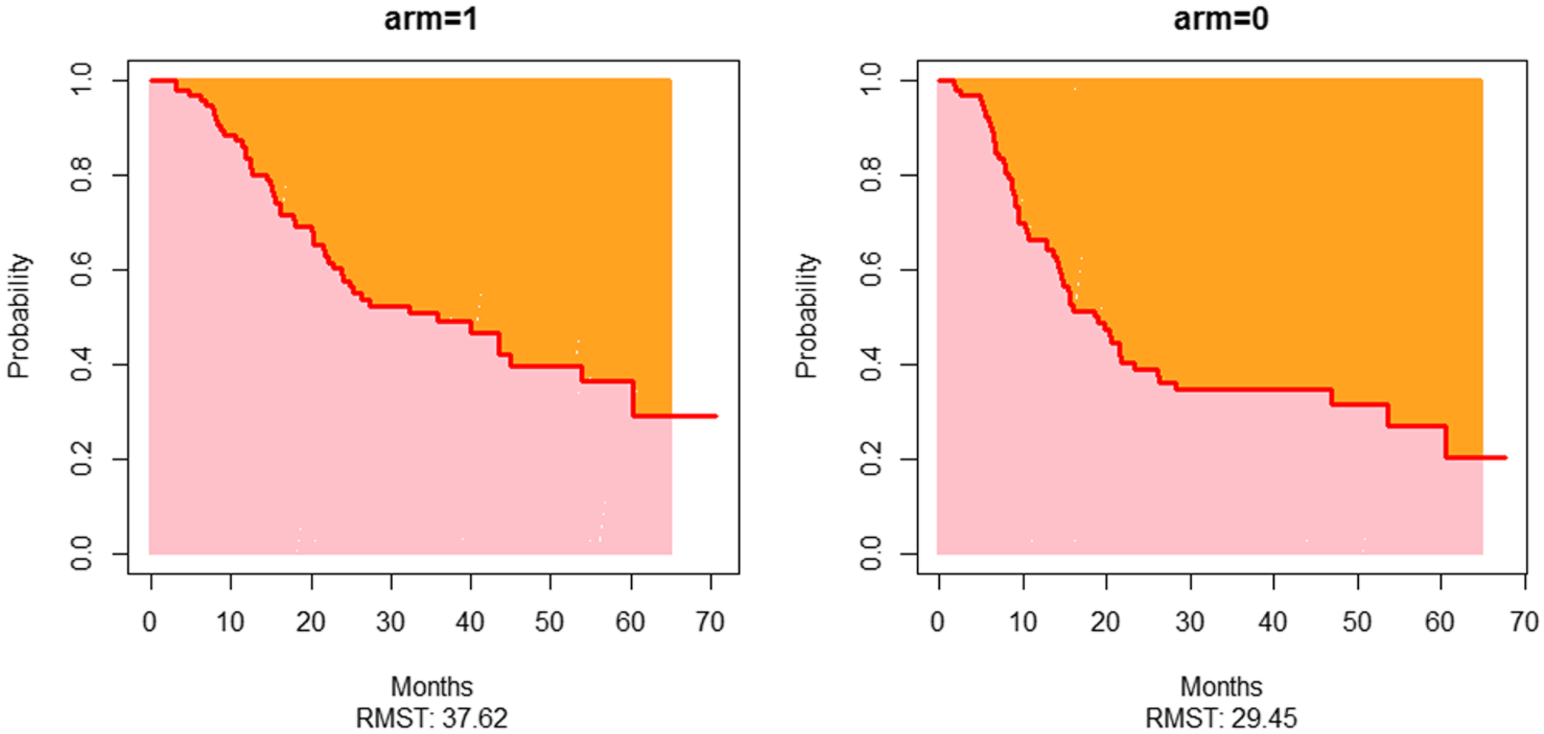
“In conclusion, the administration of metformin with or without rapamycin in patients with mPDA who achieve a response to chemotherapy is well-tolerated and was associated with better than expected overall survival in this study.”
The researchers observed “remarkably longer than expected” progression free survival and overall survival in this typically poor-prognosis population of patients. In this cohort, a low neutrophil-to-lymphocyte ratio and decreased fluorodeoxyglucose-avidity and/or decreased CA19-9 from baseline predicted improved outcomes among the long-term survivors. Overall, metformin and rapamycin were well-tolerated and their safety profiles were found to be comparable to previous reports. The researchers were forthcoming about limitations of their study—as their cohort was relatively small and the study was not powered to detect differences in clinical activity between the treatment arms.
“To this end, we identified several factors which may be used to select for patients with improved outcomes; however, whether good prognosis patients need any further treatment at all and whether poor prognosis patients will benefit from continued chemotherapy rather than a maintenance approach are not known and additional prospective studies are needed to answer these questions.”
Click here to read the full priority research paper, published by Oncotarget.

ONCOTARGET VIDEOS: YouTube | LabTube | Oncotarget.com
—
Oncotarget is a unique platform designed to house scientific studies in a journal format that is available for anyone to read without a paywall making access more difficult. This means information that has the potential to benefit our societies from the inside out can be shared with friends, neighbors, colleagues, and other researchers, far and wide.
For media inquiries, please contact media@impactjournals.com.